A case of Mandera and Wajir Counties
Background
One of the primary barriers to achieving functional community health units in Mandera and Wajir counties in Kenya is the unreliability and absence of supply chain procedures and processes. Community level stock-outs have hampered the ability of community health volunteers (CHVs) to provide the necessary health commodities and care. The root cause of these stockouts is a lack of community supply chain data visibility, which makes it difficult to predict stock-outs and create proactive and integrated community supply chain procedures and processes.
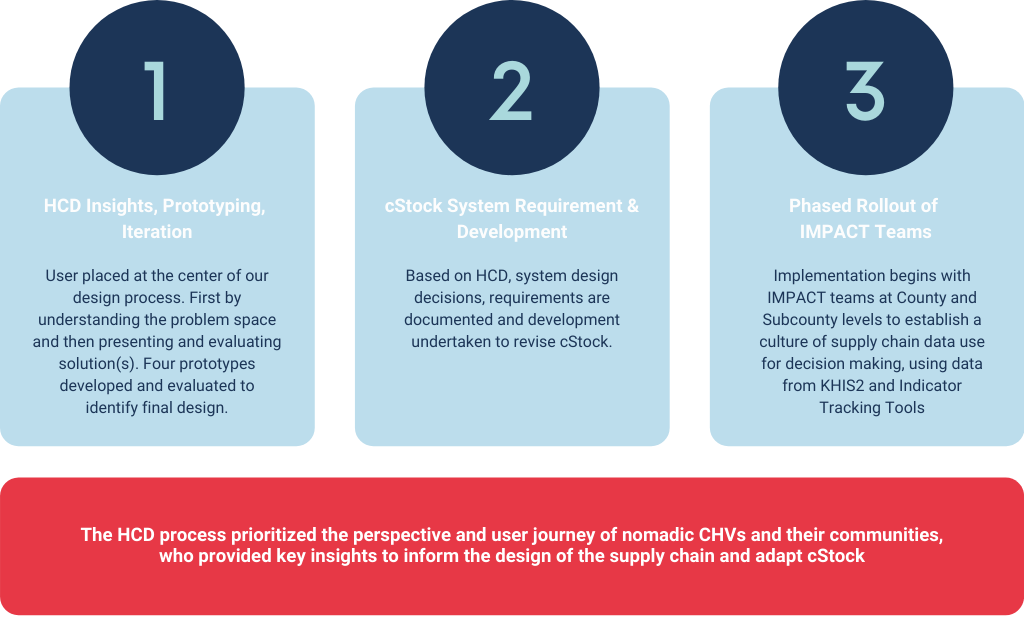
inSupply Health used human-centered design (HCD) methodology to better understand the nomadic CHVs and their communities and based on the insights gained, redesigned and adapted our proven data-centric supply chain approach, cStock, for those communities. The HCD methodology places users at the center of the design process and ensures their active participation from the beginning to the end. The cStock approach combines mobile technology, user-friendly dashboards and quality improvement teams (IMPACT Teams) to improve the visibility of logistics data at the community level to track commodities and prevent stock-outs. After the redesign, inSupply Health ensured that cStock rollout and training happened in a way that increased uptake and ownership.
Methods, tools, and processes
To generate insights, inSupply Health used one-on-one semi-structured interviews, CHV observations, and usability testing methodologies. Also, we created detailed personas, which are fictitious characters who bring to life the needs, goals, values, behavior drivers of the broader group of people, to guide our design journey. Based on our personas and our insights, we created two cStock models ensuring that we cater for differing levels of skills, motivations and contextual elements within the health system in Northern Kenya. The idea is that Model One would be a temporary phase, with CHVs and Community Health Assistants (CHAs) graduating to Model Two over the years. Our prototype included redesigned and highly visual manual tools that could be used by CHVs of all literacy levels, redesigned cStock application that considers CHVs usability constraints and includes context appropriate language, new CHA portal that will be used to test different workflows, and alternate messaging channels. See the full report on HCD research here.
cStock training and rollout
- During the cStock roll out phase, inSupply Health trained:
- 44 Sub-county Health Management Teams (SCHMT)
- 31 CHAs
- 180 CHVs from 2 counties
- 6 staff from the Save the Children
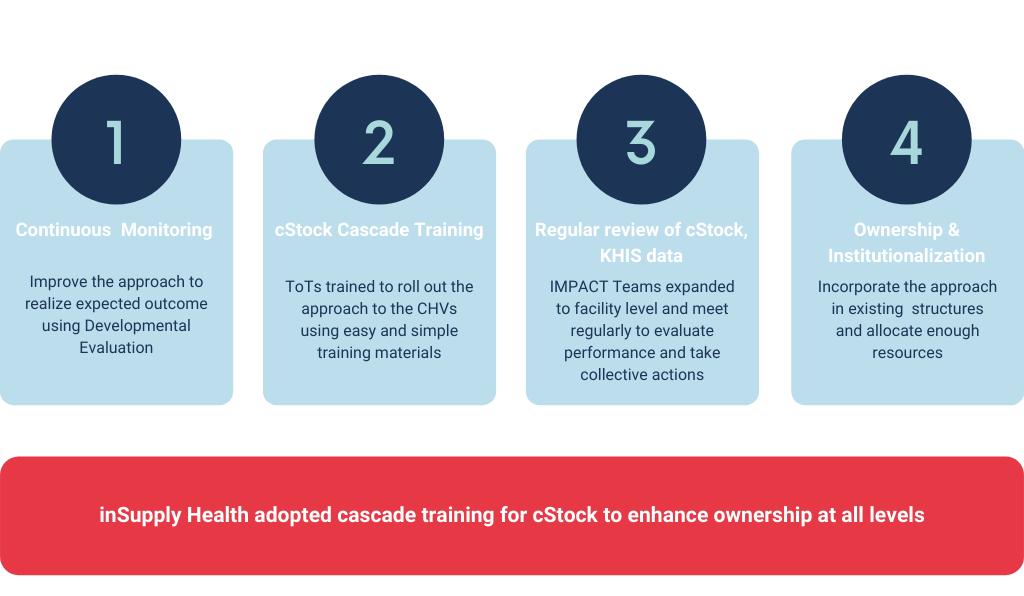
The cStock training was designed using a cascaded approach, with sub-county teams serving as master trainers to the CHAs, who in turn trained the CHVs at the community level. Cascaded training is intended to minimize the impact of staffing disruptions and external factors on cStock uptake, use and ownership that are hard to control. One of the major successes and critical factors in the platform’s uptake has been the county (Wajir & Mandera) Ministries of Health’s (MOH’s) ownership and utilization of the cStock approach with the support of a field partner, Save the Children.
Results
Despite the area’s poor network coverage and frequent movement in search of pastures and water for their livestock, nomadic CHVs have been reporting health commodities using cStock to provide real time logistics data. To accommodate the needs of the nomadic CHVs who are migrating, cStock added a feature that allows the CHAs to either assign CHVs to another link facility temporarily during migration or increase the quantities of their supplies.
Overall, the use of cStock for reporting has increased, augmenting visibility of community stock levels and providing insight into resupply processes. This has consistently helped CHAs and those who are in charge of the facilities in tracking commodities and resupplying CHVs on time to prevent stock-outs. Before using cStock, the data was reported on manual tools and not consistently submitted by CHVs. However, through cStock the CHAs are able to follow up with CHVs who have not reported and report on their behalf if CHVs are unable to report, making reporting more consistent and reliable.

Conclusion
The implementation of cStock has shown that it is a feasible, acceptable and effective solution for strengthening the fragile community health supply chains. The success of cStock implementation also shows the importance of putting users at the center of solution design. inSupply Health is continuing to explore how to evolve cStock to meet the needs of nomadic CHVs and communities in the last mile. We have partnered with Health-E-Net to integrate the PaperEMR technology into the cStock approach. The platform integration will allow nomadic CHVs to take a picture of a paper form (inventory card) and have the data automatically digitized, allowing them to overcome literacy barriers, reduce the time burden of data entry, and improve their reporting rate.